By Irshadkhan Pathan | Senior Biomedical Engineer & AI Innovator | April 2026
Reading time: 8 minutes
Table of Contents
The Problem That Frustrated Me for 20 Years
Let me paint you a picture that every biomedical professional knows too well.
It’s a Sunday night. 11PM. Your phone rings.
A ventilator in the ICU has stopped working. A patient is on ventilatory support. The on-call technician is standing in front of the machine, manual open, no idea what’s causing the fault. The AMC vendor is unreachable until Monday morning. Spare parts are not in stock. Your engineer has to drive in from home.
👉 This is exactly where AI predictive maintenance in healthcare can make the difference.
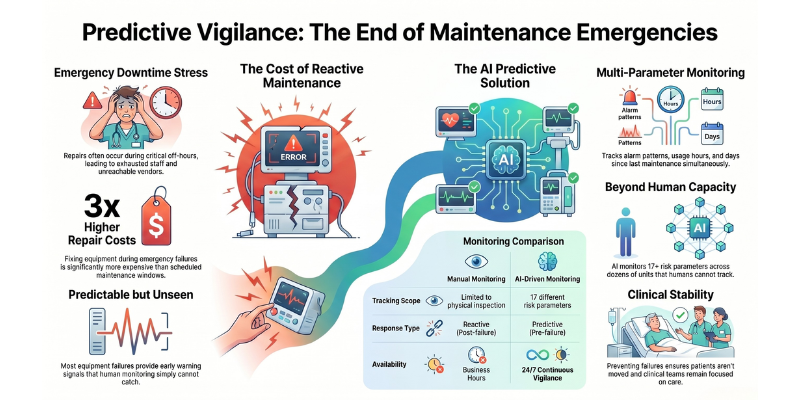
By the time the problem is resolved, it’s 2AM. The repair cost three times what it would have in a scheduled maintenance window. The patient was moved. The clinical team was stressed. And everyone is exhausted.
I lived this scenario — in different variations — for twenty years as a Biomedical Manager in a multi-specialty hospital.
Every time, the frustrating part was not the repair itself. It was the fact that the failure was predictable. If I had looked closely enough at the right signals — the alarm patterns, the usage hours, the days since the last PM — I would have seen it coming.
But nobody can monitor 22 ventilators, across multiple departments, tracking 17 different risk parameters, every single month. No human can.
So I built an AI that can.
Similar to how AI chatbots are transforming patient support in clinics, AI can also revolutionize how biomedical teams manage equipment proactively.
The Idea: Teaching a Machine What 20 Years Taught Me
Here is what two decades in biomedical management taught me that no textbook captures:
Equipment does not fail suddenly. It warns you for weeks.
Every major breakdown I have witnessed had three to five small signals before it happened. Unusual alarm patterns. Slightly longer warm-up time. Inconsistent pressure readings. We missed them because we were too busy reacting to the last crisis.
Age alone does not predict failure. Neglect does.
I have seen eight-year-old ventilators running perfectly and two-year-old ones failing constantly. The difference was never age. It was PPM compliance, usage intensity, environmental conditions — all combined. No single factor tells the story. The combination does.
👉 This is exactly why AI predictive maintenance in healthcare for medical equipment must consider multiple factors together.
The most dangerous period is just after a repair.
Counterintuitive but consistently true in my experience. Equipment serviced by an unfamiliar vendor has a higher failure rate in the following 30 days. Wrong parts, incomplete calibration, missed steps. After seeing this pattern repeatedly, I started scheduling closer monitoring of recently repaired units.
Environment is an invisible risk factor.
Room temperature fluctuations, humidity levels, power fluctuations — I have traced equipment failures back to these causes more times than I can count. But nobody tracks them systematically because they are not on any standard PPM checklist.
The failure you prevent is the one nobody talks about.
When equipment fails, everyone notices. When you quietly service a unit three weeks before it would have broken — nobody sees that. For twenty years, my most important work was completely invisible.
I realised that if I could encode everything I knew — all these patterns, all these signals — into an algorithm, it could monitor every ventilator simultaneously, every month, and tell me which ones needed attention before they failed.
That became the project.
What I Built: The AI Ventilator Breakdown Prediction System
The Goal
A system that scans all ventilators in the hospital every month, analyses risk across multiple parameters simultaneously, and produces a priority-ranked report — flagging which machines need proactive maintenance before they fail.
The Technology
I am a Biomedical Manager, not a software engineer. So I made deliberate choices to keep the technology accessible:
- Language: Python 3.13 — the industry standard for AI development
- Algorithm: Random Forest Classifier with 300 decision trees
- Libraries: scikit-learn, pandas, numpy, joblib — all open source, zero cost
- Training data: 100 ventilator profiles across diverse departments and brands
- Execution: A simple Windows batch script — double-click to run
- Storage: Hospital shared drive — no cloud, no internet required, data never leaves the hospital
- Output: A timestamped CSV report and automatic audit log — fully NABH compatible
The entire system was built in-house. No vendor. No external consultant. No ongoing licensing fee.
Why Random Forest?
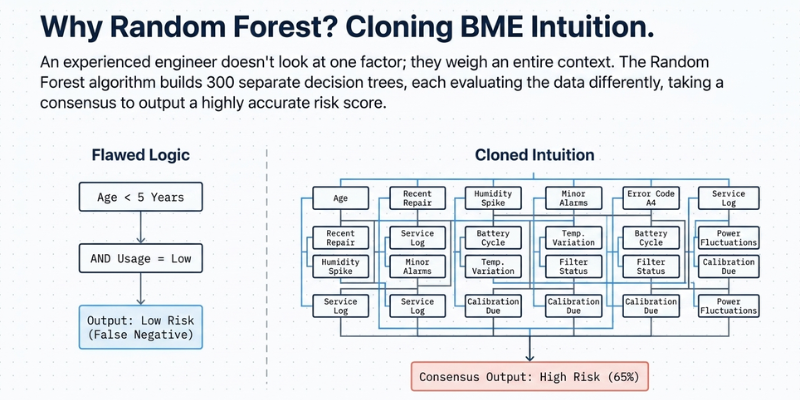
I chose the Random Forest algorithm specifically because it mirrors how an experienced engineer thinks.
An experienced BME professional does not look at one factor and make a decision. They look at age, usage, maintenance history, recent alarms, environmental conditions — and they weigh all of them together before forming a judgment.
Random Forest does exactly this. It builds 300 separate decision trees, each one evaluating the data differently, and then takes a consensus. The result is a breakdown probability score that accounts for the interaction between all risk factors — not just individual ones.
The 17 Parameters: What the AI Measures
This is the core of the system. I spent months deciding which parameters to include, drawing directly from my clinical experience of what actually predicts failures.
Equipment Status
- Equipment age in years
- Total usage hours
- Usage hours in the last month
Maintenance History
- Days since last preventive maintenance
- PPM overdue days
- Annual maintenance cost
- AMC vendor response time
Failure Signals
- Number of breakdowns in the last 6 months
- Critical alarm count
- Overall uptime percentage
Environmental Factors
- Average room temperature
- Average humidity
- Frequency of power fluctuations
- Sensor age
Operational Data
- Department type (ICU, ICCU, CATH, ER carry different risk profiles)
- Maintenance compliance score
- Last breakdown severity rating
The AI cross-analyses all 17 parameters simultaneously for every ventilator — something that is simply impossible to do manually for 22 machines every month.
How It Works: The 3-Step Process
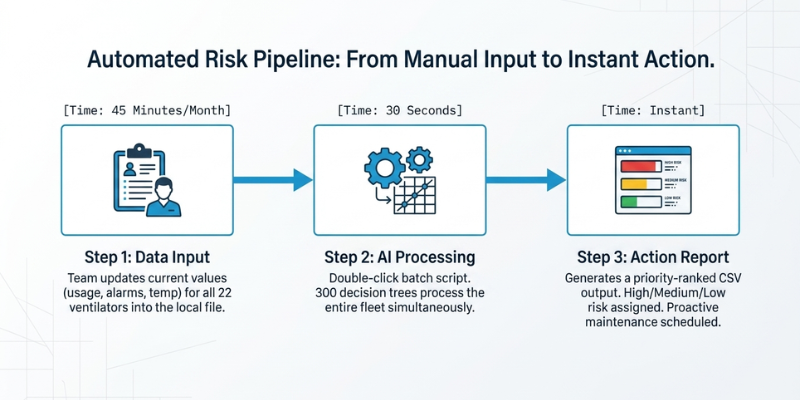
Step 1 — Data Collection (Monthly)
Each month, my team updates the data file with current values for every ventilator. Equipment age, usage hours, PM history, alarm counts, temperature and humidity readings, vendor response times. This takes approximately 45 minutes for all 22 ventilators.
Step 2 — AI Model Analysis (30 Seconds)
Double-click the batch script. The Random Forest model reads the data, runs all 22 ventilators through 300 decision trees each, calculates breakdown probability scores, and generates a priority-ranked report. The entire process takes under 30 seconds.
Step 3 — Action Report (Instant)
The output is a ranked list showing every ventilator with its breakdown probability percentage and risk level — High, Medium, or Low. The engineer reviews the top-risk units and schedules proactive maintenance immediately. A timestamped audit log is created automatically for every run.
No internet required. No login. No subscription. Just data in, risk report out.
The March 2026 Results: First Live Prediction Run
In March 2026, we ran the system for the first time on all 22 ventilators in our multi-specialty hospital.
The results were striking.
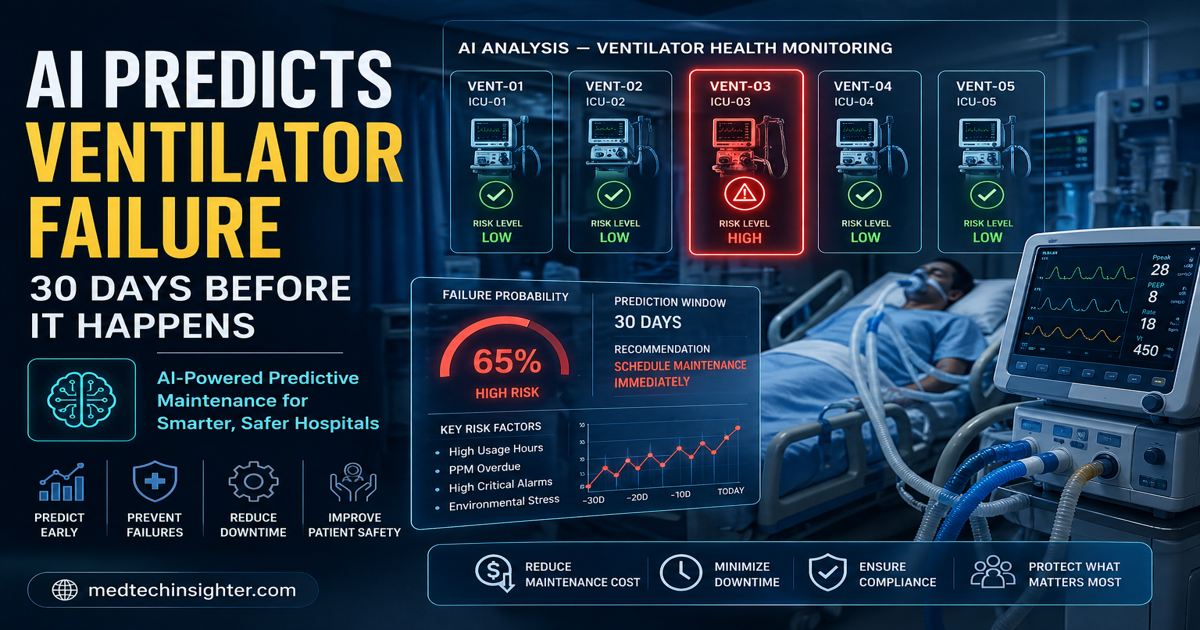
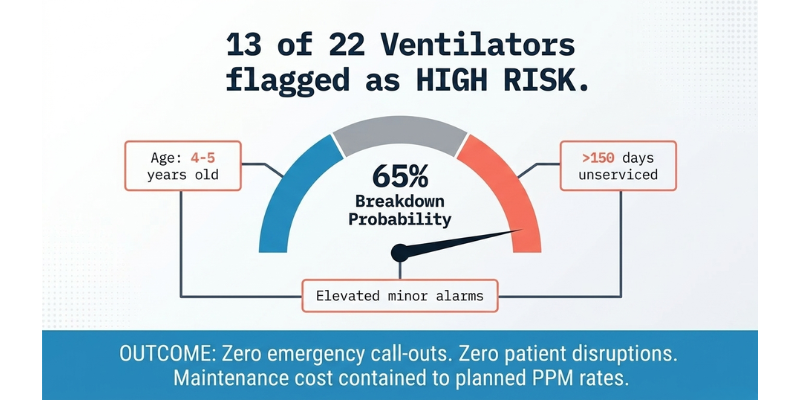
13 out of 22 ventilators were flagged as HIGH RISK.
The top-ranked unit showed a 65% breakdown probability. The next three units in the ICCU showed probabilities between 57% and 63%.
On reviewing the data, the pattern was clear. These units shared three common risk factors: they were 4-5 years old, they had not been serviced in over 150 days, and they had accumulated elevated alarm counts over the previous 6 months. No single factor was alarming on its own. Together, they painted an unmistakable picture.
We immediately scheduled proactive maintenance for all high-risk units over the following two weeks.
The outcome:
- Zero emergency call-outs for any of the flagged units
- Zero patient disruptions
- Maintenance cost remained at planned PPM rates — not emergency repair rates
- Every prediction run created an automatic NABH-compatible timestamped audit log
The prevention was no longer invisible. It was documented.
Why This Matters Beyond Our Hospital
This system addresses three problems that every hospital in India faces.
Patient Safety
Ventilators are life-critical equipment. A failure during active patient use is not just a maintenance problem — it is a patient safety incident. Predicting and preventing that failure is the most direct form of patient protection a biomedical department can provide.
NABH and JCI Compliance
The FMS.4 and FMS.4.2 standards require documented, risk-based maintenance programs. Every prediction run our system generates creates an automatic timestamped audit log — exactly the kind of evidence NABH auditors look for. Predictive AI maintenance is not just operationally better. It is compliance documentation built into the workflow.
Cost Reduction
Emergency repairs cost three to five times more than planned preventive maintenance. Beyond the direct repair cost, unplanned downtime affects department capacity, staff scheduling, and patient throughput. The financial case for predictive maintenance is straightforward — and the system costs nothing to build if you have the knowledge and the data.
What Comes Next: The Roadmap
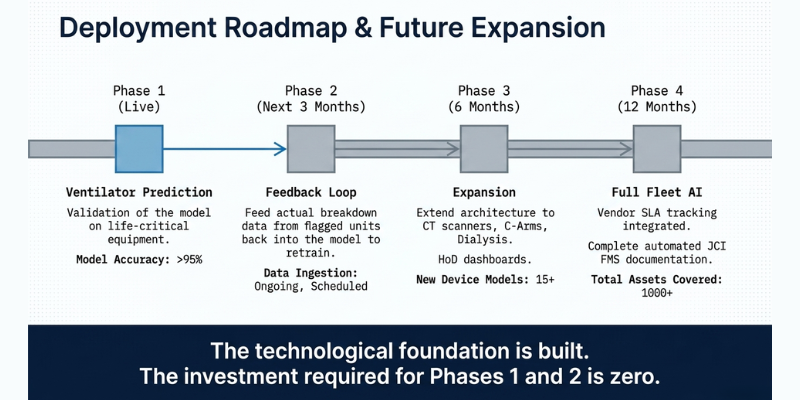
The ventilator prediction model is Phase 1. The same architecture extends to every major piece of equipment in the hospital.
Phase 2 (Next 3 months): Feed actual breakdown feedback from the flagged units back into the model. Retrain with real outcome data. Improve prediction accuracy.
Phase 3 (6 months): Extend the model to CT scanners, C-Arms, and dialysis units. Build a department-level dashboard for Heads of Department.
Phase 4 (12 months): Full fleet AI coverage. Vendor SLA tracking integrated into the risk model. Complete JCI FMS documentation generated automatically.
The investment required for Phases 1 and 2 is zero. The same knowledge and tools that built the ventilator model apply across the entire hospital fleet.
What Any Biomedical Professional Can Learn From This
You do not need a computer science degree to build something like this.
What you need is domain expertise — the deep knowledge of what actually causes equipment to fail in your specific environment. That knowledge is worth more than any algorithm. The algorithm is just the tool that acts on it at scale.
If you have spent years watching equipment fail and quietly knowing why — that pattern recognition is the most valuable input any AI model can have.
The path I took:
- Identified the problem clearly — reactive maintenance was costing us time, money, and patient safety
- Defined what I already knew — the risk factors I had been tracking mentally for years
- Learned just enough Python to build the model — there are excellent free resources for this
- Started with one equipment type — ventilators, because they are the highest risk
- Used real hospital data — not simulated or hypothetical
- Built for simplicity — double-click operation, shared drive storage, no internet dependency
The result is a system that any biomedical department can replicate, with their own data and their own equipment knowledge.
Final Thought
For twenty years, my best work was invisible.
The equipment that never failed. The patients who were never disrupted. The emergencies that never happened — because someone serviced a machine three weeks before it would have broken.
AI does not replace that work. It makes it visible. Documented. Measurable. Undeniable.
That is what this system does. And that, more than any technical achievement, is what I am most proud of.
Irshadkhan Pathan is a Senior Biomedical Engineer and AI Innovator with 20 years of experience in multi-specialty hospital management. He writes about AI in healthcare, biomedical equipment management, and the future of predictive maintenance at medtechinsighter.com.
Did this post help you? Share it with one biomedical professional who needs to read it.
Tags: Biomedical Engineering, AI in Healthcare, Predictive Maintenance, Hospital Management, Ventilator Maintenance, NABH Compliance, MedTech, BME, ChatGPT, Machine Learning in Healthcare